




Digital tools are improving data quality, and use of data for decision-making in indoor residual spraying campaigns, malaria case investigations, and general malaria surveillance.
A famous management consultant and organizational theorist once said that “without big data, you are blind and deaf in the middle of a freeway.” While these words were said in a different context, they could not be truer for countries pursuing malaria elimination around the world. Countries in malaria elimination settings are doing the work to reduce transmission, but do they have effective surveillance system structures that can support the data driven decision-making that is necessary to eliminate the disease for good?
Surveillance systems are the backbone of successful malaria programs as the information they collect is essential for the design, implementation, and monitoring and evaluation (M&E) of interventions. The World Health Organization’s (WHO) Global Technical Strategy for Malaria 2016-2030 recommends for countries to adopt malaria surveillance as a core intervention, to strengthen their electronic information systems for surveillance to improve the timely delivery of quality information, and motivate data-driven decision making.
 Discovering common challenges across the region
Discovering common challenges across the region
When CHAI started working in health informatics in Central America and Hispaniola in 2017, surveillance as a core malaria intervention was lagging across the five countries we work with: the Dominican Republic, Guatemala, Honduras, Haiti, and Panama. Through a situational evaluation study, we discovered common challenges among these countries, which included:
- A lack of malaria-specific electronic surveillance systems in each country: Malaria surveillance was paper-based, resulting in delays to access to information, limiting timely decision-making.
- Multiple parallel information systems that increased the data collection workload, thereby delaying data analysis due to data inaccessibility.
- Limited data use for implementing outbreak responses and targeted interventions for improved progress towards elimination.
Following the study, we set out to address the challenges and improve the malaria surveillance systems of these countries. With support and acquired knowledge from CHAI’s global malaria and other regional teams, we developed standard operating procedures, training materials, tools and dashboards in collaboration with the different ministries of health to ensure capacity building, ownership and sustainability of the projects.
Success stories in Honduras, Panama, and Guatemala
To date, the biggest achievements CHAI has propelled in the region are the implementation of the national health information system in Honduras, the pilot and scale up of the malaria module in Panama and the development of the malaria module in Guatemala. CHAI has also supported the implementation of tools to streamline the data collection and analysis of vector control activities, community health worker networks, and entomological surveillance.
In Honduras, with CHAI support, the ministry of health implemented SIIS (Health Information Integrated System in Spanish) which is based on the DHIS2 platform – an open source, web-based health management information system used in over 70 countries for malaria and other diseases. Currently, SIIS is completely institutionalized and operational nationwide. It is used in other health areas beyond malaria, which increases sustainability and represents a big success for the country.
In 2019, Honduras reported fewer than 500 cases, the vast majority of which came from remote and hard to access areas of the country. The information system was adapted to promptly collect precise, high quality, timely, and complete data from areas with poor accessibility and almost no connectivity. CHAI supported the development of the mobile DHIS2 Android capture application, bringing the data entry point closer to the source of information. To date, case notification and investigation, including geolocation, are reported by 61 mobile devices deployed in five regions. Extensive training and support have been key to a successful implementation; CHAI and the MoH work together in regularly upgrading the platform to improve its automation, visualizations, and data quality control capabilities. As a result of the deployment of the new digital tools, in-field trainings and supervision visits, case classification rates increased from 81 to 92 percent and case investigation rates bumped up from 81 to 93 percent from August-October to November-December
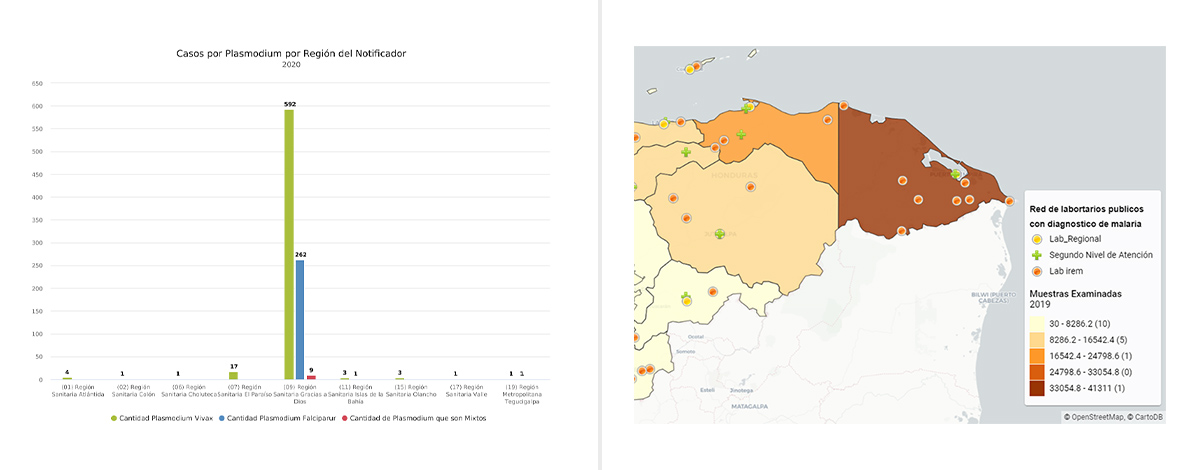
Fig. 1 Examples of dashboard visualizations, on the left malaria cases by plasmodium and on the right number of tested samples, Honduras 2019.
Panama is a good example of a country where malaria surveillance was completely paper based and data was not being digitized. This caused so many delays in collecting and analyzing the information that data was often not even used for decision making. Moreover, data management was controlled by the head office with no feedback to other levels, forcing regions to maintain and manage their own databases, which led to inconsistencies in reporting.
To improve the situation, the ministry of health – alongside CHAI – developed a malaria-specific module within the national surveillance system with a dashboard that shows key indicators for malaria surveillance, epidemiological situation, and case management. The module, which is now implemented in five out of fifteen regions of the country, collects complete data on malaria cases, including their notification, treatment, classification, investigation, and all patient follow-up. Cases can be analyzed by any of the organizational units of the country, including locality, foci, region, state or province. The definition of an official locality list added to the design of the module, as having the possibility of accessing data on a general or more granular level facilitated a more effective adjustment of strategies in respect to community or country needs.
As a result of the use of the module, the number of cases notified, active users, number of classified cases, rate, and laboratory reports submitted have all improved. National scale up of the module is scheduled to be completed by the first quarter of 2021.
Furthermore, CHAI is in the process of implementing DHIS2 to manage information from vector control interventions, such as Indoor Residual Spraying (IRS) and bed net distribution. This tool was recently piloted with good results and will also be scaled up nationally in 2021.
In Guatemala, CHAI introduced a mobile IRS data collection app in Escuintla, the country’s most endemic malaria region, to support regional vector control efforts. This tool has over 6,000 houses from 12 localities registered and has been used in two annual IRS campaigns for vector control operations to monitor spray coverage and insecticide use rate to ensure that targets are met. The app has dashboards with simple visualizations, tables, and maps that provide real-time data analysis. The biggest benefit of the app for the teams is having access to information quickly, providing the opportunity to better manage spray team operations, make decisions about insecticide consumption and monitor coverage. The tool will be extended to support the bed net distribution and evaluation.
CHAI, with the support of the ministry of health, also piloted a malaria electronic surveillance system in Escuintla. Once approved by the government, the system will integrate information used by both the national malaria program at national and local levels, as well as the national Department of Epidemiology. It will include information on suspected and confirmed malaria patients from case detection to investigation, treatment, and follow-up. The module will, for the first time, allow lab technicians to input information directly into the electronic system, enabling robust data collection and analysis from different end users.

Fig 3. Example of IRS dashboard in Guatemala, map of a community targeted to receive IRS with households shown by current spray status
Looking to the future
These are some of the ways that CHAI has strengthened malaria surveillance to support malaria elimination in the region. To ensure that the gains made over the next few years are sustainable, CHAI will now focus on building government capacity to use these electronic surveillance tools for evidence-based decision-making to improve and target interventions to the right places and at the right times. We will continue working alongside our government counterparts to design solutions they want and need, while ensuring they have the resources to implement them.
Reaching malaria elimination is not an easy task, but with strong surveillance and health informatics systems in place, the path is clearer, and the goal within reach.
Contributing writers: Bernardo Garcia Espinosa (Research Associate, Mesoamerica), Melissa Wiles (Research Associate, Mesoamerica), Sarah Park (Research Associate, Mesoamerica), Justin Lana (Analytics and Surveillance Technical Advisor, Global Malaria), Daragh Gibson (Technical Advisor, Global Malaria), Abrahan Matias (Senior Associate, Global Malaria), Lakshmi Balachandran (Associate Director, Global Malaria).
