




INTRODUCTION
The quality of data on routine immunization (RI) in Nigeria has been a long-standing concern for the government and its partners. In 2017, the RI module of the District Health Information System (DHIS2)—an open-source, web-based platform—was rolled out in Nigeria. It was adopted as the sole reporting platform for RI data in 2018. Over time, significant data quality issues have come to light, especially when comparing data from the platform to household surveys such as the National Demographic and Health Surveys (NDHS), which are regarded as the gold standard for immunization coverage estimates[1]. For instance, in 2018 the DHIS2 showed that 79 percent of children had been vaccinated with pentavalent 3 in Lagos state, whereas the NDHS reported 91 percent of children covered[2]—a data disparity that is above the acceptable threshold of 10 percent[3].
RI data quality issues have been grouped into three categories: technical, organizational, and behavioral[4]:
- Technical factors affect the structure and the design of the Health Management Information System (HMIS), as well as information flow. Issues such as limited internet availability, no data bundles to access the internet via a mobile device for data entry at the local government area (LGA) level, and capacity gaps in RI data management among healthcare workers (HCWs) at LGA and health facility (HF) levels are common themes.
- Organizational determinants influence the context in which RI data collection, management, and use occur. Typical examples include weak routine immunization supportive supervision (in both scope and quality) and poor supervision of conduct and quality of RI data validation and review meetings at the LGA level.
- Behavioral issues related to collection, management, and use of RI data. These issues include the poor attitudes toward data recording and reporting and the use of data for decision making, as well as poor data use during and after the delivery of RI services.
As part of CHAI’s work to increase data accuracy and use for decision-making at national and state levels, we supported the Lagos State Primary Healthcare Board (LSPHCB) with the development and implementation of a data quality improvement plan (DQIP) (See Figure 1 below).

Figure 1: Process for Data Quality Improvement Plan (DQIP)
CONTEXTUALIZING THE NATIONAL DQIP FOR LAGOS STATES
Development
Consolidating work done at the national level, CHAI carried out desk reviews of existing strategic documents to identify and adapt interventions to be infused into the government’s improvement plan. Plenary reviews with the government, donors, and partners were conducted to assess and prioritize strategies and interventions based on their feasibility, the availability of existing structures or processes, and funding. RI data quality used for decision making will improve, and consequently result in a more efficient immunization program if the DQIP is developed with the following objectives:
- Strengthen data entry and analysis practices and processes at LGA and HF levels.
- Enforce accountability measures among healthcare workers on RI data management at all levels.
- Enhance the conduct of supportive supervision and on-the-job mentoring at LGA and HF levels.
- Strengthen the conduct of monthly RI review and validation meetings at the LGA level.
Implementation
Between 2019 and 2020, the DQIP was disseminated to key officials of the LSPHCB at the state level, as well as managers at the LGA level. Following this dissemination, the state began implementing the DQIP with the support of CHAI and other development partners. The process ensured domestication and state ownership of DQIPs, including updating date training and orientation for health workers, dissemination of the accountability framework with all stakeholders (state and LGA level), and conducting refresher training for supervisors to review state and LGA data validation procedures. In addition, it involved the development of standard operating procedures (SOPs) for data validation and review meetings, and the development of primary healthcare (PHC) data management dashboard for state-level monitoring and evaluation (M&E) officers of the LSPHCB.
CHAI supported Lagos State to build the dashboard to ensure effective and efficient monitoring of essential PHC services, data quality, and the use of data for decision-making and implementation.
Figure 2: Landing page of the PHC Dashboard
Figure 3: Data entry page of the PHC dashboard
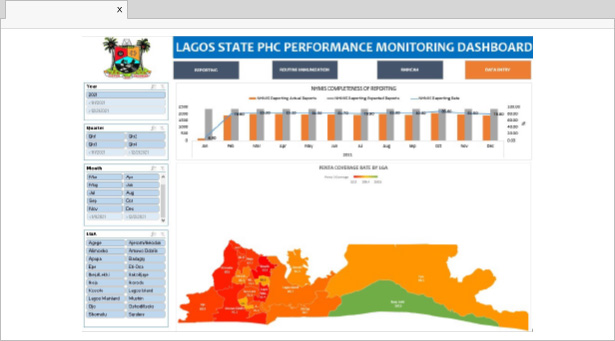
Figure 4: Routine immunization dashboard showing some of the available charts
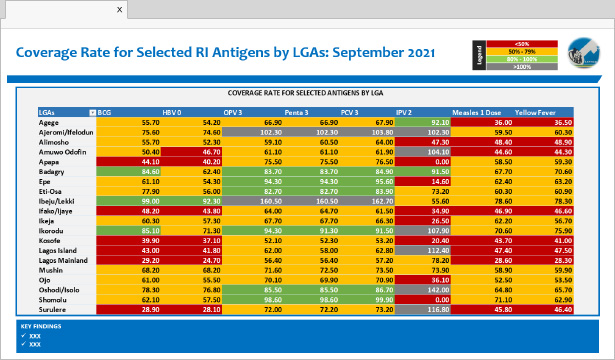
Figure 5: Presentation based on visualization from the dashboard
Following the development of the dashboard with key inputs from the Directorate of Monitoring and Evaluation, the state M&E officers were upskilled in the use of the updated dashboard. The team utilized the insights from this tool to drive monthly data meetings and influence quarterly management meetings at the PHCB level.
MONITORING & EVALUATION
In October 2021, CHAI supported the state to develop a checklist to optimize the monitoring of state performance against the operationalization of the DQIP. As of Q4 2021, through the diligent efforts of the state, supported by CHAI and development partners—60 percent of activities were completed, despite challenges such as COVID-19 vaccination campaigns and funding constraints.
In addition to highlighting the status of the DQIP, the checklist served as an advocacy tool for the state to prioritize data quality efforts. This led to an increased completion rate of 63 percent as of Q1 2022. Furthermore, while we are seeing improvements in data management coordination and accountability, these efforts are also contributing to improvements in data quality. For instance, the timeliness of National Health Management Information System (NHMIS) data reporting for the state has increased from 57 percent in February 2021 to 76 percent in February 2022. Similarly, the timeliness of the Health Facility Vaccine Utilization Summary increased from 34 percent in February 2021 to 80 percent in February 2022 [5].
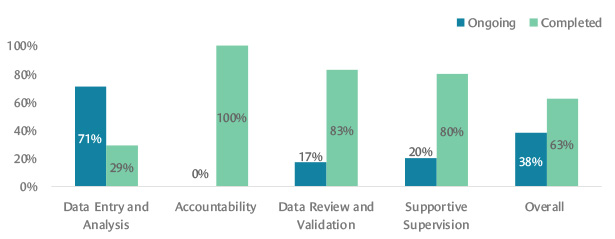
Figure 6: Implementation status of DQIP as of Q1 2022
THE WAY FORWARD
It is important to ensure continuous tracking of the operationalization of the DQIP across the state. One recommendation is to include activities highlighted in the DQIP in the RI and LSPHCB annual operational plan (AOP). The checklist would also be reviewed at quarterly review meetings. The chances of success are higher by leveraging existing platforms and integrating these activities.
The journey to clean, accurate, and reliable data for implementation is ongoing and Lagos state is moving in the right direction. Like any journey, there have been challenges that threatened to impede the work such as:
- Competing priorities can hinder the operationalization of some core activities.
- Inadequate funding to support the implementation of some recommended interventions.
- Administrative issues with DHIS2 that affect the completeness of data.
However, with the level of commitment the state has shown, alongside continuous support from partners, the goal of achieving quality data for decision-making and implementation is within reach.
This work was done in collaboration with the Lagos State Ministry of Health and Lagos State Primary Health Care Board and was supported by funding from the Bill & Melinda Gates Foundation.
Contributing authors: Dr. Shola Dele-Olowu, Deputy Director, Vaccines Program; Akachi Mbogu, Manager, Immunization Systems & Capacity; Dr. Sebastian Ilomuanya, Manager, Immunization Management Systems and Capacity, Global Vaccines; Dr. Owens Wiwa, EVP Global Resources for Health, West and Central Africa and Country Director Nigeria.
[1] Nigeria Routine Immunization Data Quality Improvement Plan (DQIP: 2019 – 2023)
[2] National Demographic and Health Survey: 2018, ICF International and USAID.
[3] For the 2017 birth cohort, survey coverage data is sourced from NDHS 2018. Survey data samples children aged 12-23 months, while admin data samples children aged 0-11 months
[4] Nigeria Routine Immunization Data Quality Improvement Plan (DQIP: 2019 – 2023).
[5] DHIS2: accessed 24 March 2022

